Area differences in healthcare utilization have been documented since an area variation analysis of tonsillectomy rates was published back in 1938. Besides the research literature, geographic variation in U.S. healthcare also has been documented extensively for the Medicare population in the Dartmouth Atlas. The Institute of Medicine also released a series of reports on geographic variation in healthcare spending in early 2013. General consensus from these studies is that significant regional difference in various health services is observed after adjusting for available patient and payer differences.
Regional variation in healthcare utilization is greatest among procedures or diagnoses with variation in standard practices. Syncope, for example, can be treated efficiently on an ambulatory basis or in the inpatient setting up to 1 day. It largely depends on physicians’ preference as to whether to treat a syncope patient outside the hospital or keep the patient overnight. The chart below illustrates the regional difference in Emergency Room and/or Observation Care (“ER/OBS”) utilization and inpatient admissions for syncope between four New York and New Jersey plans and four California plans. Data for all plans are limited to commercial members, and utilization rates are adjusted to reflect standard commercial demographics. Compared to the commercial average (regression line), the four California plans stay at the lower ends of both ER/OBS visits per 1000 and inpatient admission via ER/OBS per 100. On the contrary, the four New York/New Jersey plans not only had a higher than average rates of syncope ER/OBS visits but also admitted a higher percentage of syncope patients via ER/OBS to the inpatient setting.
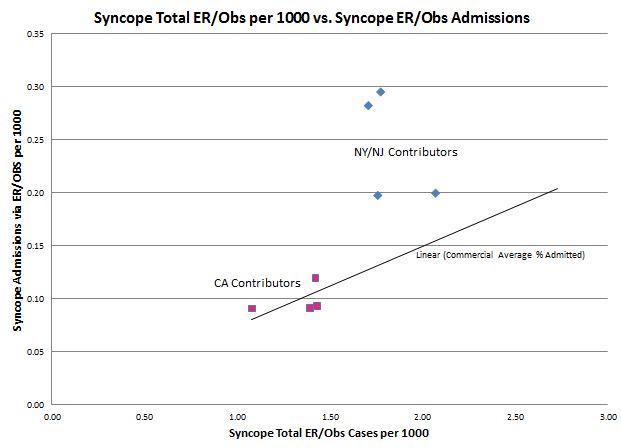
The difference in ER/OBS visits rate between the California plans and the New York/New Jersey plans for syncope perhaps reflects not only where syncope patients seek care in different areas but also the availability of primary care sources in each area. It may also reflect different patient understandings of the appropriate role of Emergency Department care. However, the difference in the syncope ER/OBS admission ratio (syncope admissions via ER/OBS per 1000 divided by syncope ER/OBS visits per 1000) reflects more on differences physician decision-making. For this condition, physicians in New York/New Jersey admitted ER/OBS syncope patients to the inpatient setting much more often than those in California did (9.6% – 16.6% vs. 6.5% – 8.4%). Even assuming that the same diagnostic work-up takes place in either the inpatient or the outpatient setting, the added cost of accommodating this much higher percentage of patients overnight in the hospital can be substantial.
The methodology embedded in the MedInsight Guideline Analytics software solution was used to create the analysis for this article, e.g. the definition of syncope in medical claims data and the means to count admits, observation, and ER cases.