Coronary angiography is a key diagnostic tool in the management of patients with coronary artery disease. Coronary angiography is used to identify narrowing in coronary arteries and is used for decision support to ascertain the need for revascularization to minimize the risk of myocardial infarction. Various research studies have evaluated trends in the use and results of coronary angiography as key contributory factors to the variations seen in rates for coronary revascularization across the US. For example, a large study by Chan, et al. highlighted that inappropriate revascularization rates ranged from 0% to 55% in different facilities. The use of diagnostic angiography has been advocated in different guidelines to ensure that the revascularization is warranted, however, this approach does not address inappropriate selection of patients for a diagnostic angiography.
According to the American Heart Association (AHA), coronary angiography is not recommended in patients who are at low risk according to clinical criteria and who have not undergone prior non-invasive risk testing. Coronary angiography is also not recommended in asymptomatic patients with no evidence of ischemia or non-invasive testing. However, various studies observe that current practice patterns are not consistent with these recommendations. Abdallah, et al. in their review of the National CathPCI registry found that, out of 790,601 elective coronary angiographies performed on patients with no history of Coronary artery disease (CAD), approximately 291,586 angiographies were not preceded by any stress test. Amongst these patients with no stress test prior to coronary angiographies, approximately 38.5% did not have symptoms of angina.
Other studies have highlighted the variable diagnostic yield of elective diagnostic angiographies. A 2010 Patel et al. study of the cardiovascular national registry found that, in patients without known heart disease who underwent elective invasive angiography, 37.6% had obstructive coronary artery disease. This implies that nearly two-thirds of patients had a negative result for obstructive coronary artery disease. Amongst the group with no obstructive heart disease, 30.0% were noted to have no symptoms, including no angina.
False positive findings in inappropriate diagnostic tests can trigger subsequent treatment. Referred to as “diagnostic-therapeutic cascade,” inappropriate angiography in asymptomatic patients increases the likelihood of performing inappropriate coronary artery revascularizations and other associated medical utilization. Bradley, et al. studied 544 hospitals that performed more than 1 million elective coronary angiograms and more than 200,000 elective percutaneous coronary interventions (PCI) between 2009 and 2013, and found that 25.1% of patients were asymptomatic at the time of angiography. The proportion of angiographies performed on asymptomatic patients by individual hospitals ranged from 1% to 73.6%. Hospitals with higher rates of angiography performed on asymptomatic patients also had higher rates of inappropriate PCIs and lower rates of appropriate PCIs.
Considering the volume and cost of these procedures, it is important to reinforce appropriate patient selection for coronary angiography.
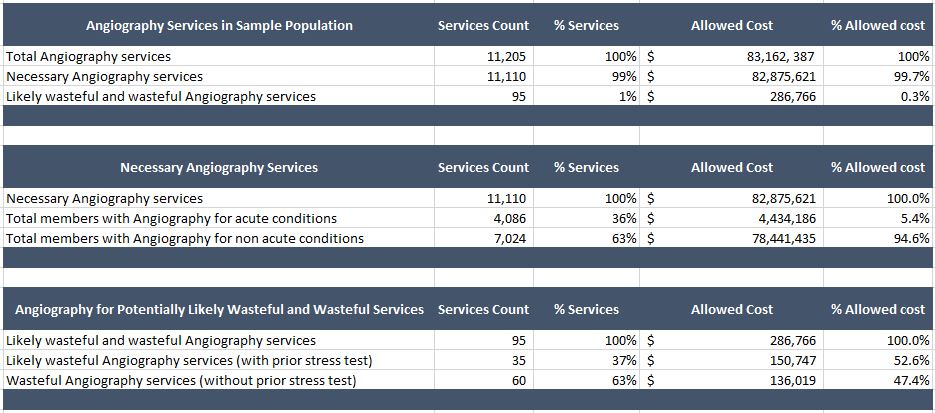
To study the practice pattern of coronary angiography and associated services, we reviewed administrative claims data of a Midwestern US Health plan for the July 2011-June 2012 time period. MedInsight’s Health Waste Calculator tool was used to identify necessary, likely wasteful, and wasteful angiography service units. Angiography services for members who had administrative data evidence for cardiac symptoms or high risk diagnosis (ischemic and coronary heart disease, diabetes, and peripherally artery disease) were assigned as necessary services. The analysis in Table 1 shows that 99% of angiography services (n=11,110) met the necessary criteria, while 1% of services were determined to be either likely wasteful or wasteful (n=95), having no evidence for the presence of any the underlying symptoms or diagnosis that would classify these as necessary.
Further analysis highlighted that, amongst the necessary services, 37% were conducted for acute conditions (acute coronary syndrome, angina, and myocardial infarction), while 63% of services were conducted for non-acute conditions. Amongst the inappropriate angiography services, 37% of members received a cardiac stress test prior to the angiography, whereas the remaining 63% of members did not. Due to the absence of clinical data, such as from an Electric Medical Records (EMR) system, we assigned the non-necessary services with a prior stress test as “Likely Wasteful” and the remaining services with no prior stress test as “Wasteful.”
Table 1: Profile of Angiography Services
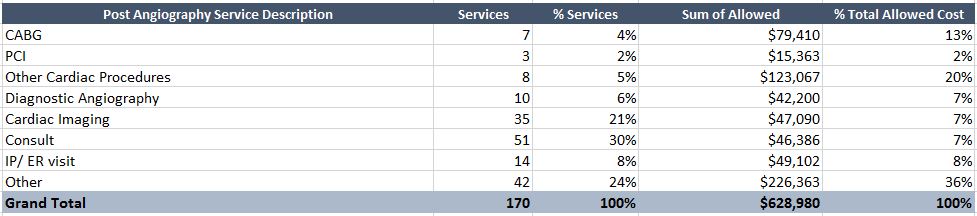
To study if members with wasteful angiography had other associated costs of follow-up and cardiac revascularization, we reviewed the utilization experience of members with wasteful angiography services for a period of six months after the wasteful service date. Table 2 summarizes the results of this analysis. We restricted our analysis to utilization for cardiac-related procedures and encounters. We found that cardiac revascularizations (including CABG and PCI) and other cardiac procedures comprised 11% of all cardiac related services, with a combined cost of $217,840 (35% of all allowed cardiac related costs). Follow-up diagnostic angiographies and cardiac imaging comprised another 27% of cardiac related services, with a combined cost of $89,290 (14% of all allowed cardiac related costs).
Table 2: Post-Angiography Utilization by Members with Wasteful Services
While the results of this analysis are consistent with the low end of what has been reported for inappropriate coronary angiographies (1% to 73.6%) it raises concern over the need to improve patient selection for coronary angiography. It is important to note that claims data alone is not sufficient to identify wasteful angiography services with absolute certainty. However, even with conservative estimates, these findings confirm the significant resource use and expenses after angiography and the potential medical waste in the subsequent period.
Sources
Chan et al, Appropriateness of Percutaneous Coronary Intervention JAMA. 2011;306(1):53-61. Available at: https://jama.jamanetwork.com/article.aspx?articleid=1104058
Jeffery L Anderason, Jonathan L. Haperin. “Guideline for the Diagnosis and Management of Patients with Stable Ischemic Heart Disease”; Journal of the American College of Cardiology. 2012; 60(24):2564-2603. Available at https://content.onlinejacc.org/article.aspx?articleid=1391403
Mouin S. Abdallah, John A. Spertus. “Symptoms and Angiographic Findings of Patients Undergoing Elective Coronary Angiography Without Prior Stress Testing”; American Journal of Cardiology. Available at https://www.ajconline.org/article/S0002-9149(14)01112-6/pdf
Manesh R. Patel, Eric D. Peterson. “Low Diagnostic Yield of Elective Coronary Angiography”; New England Journal of Medicine 2010 March 11; 362(10): 886–895. Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3920593/pdf/nihms540259.pdf
Bradley SM, Spertus JA. “Patient selection for diagnostic coronary angiography and hospital-level percutaneous coronary intervention appropriateness: insights from the National Cardiovascular Data Registry”; JAMA; 2014;174 (10):1630-1639. Available at https://archinte.jamanetwork.com/article.aspx?articleid=1898877